Good Pain vs Bad Pain During Training: How to Tell the Difference

Resistance training requires individuals to lift heavy weights often, with the purpose of inducing mechanical (bone, joints etc.) and/ or physiological (muscle) changes. Essentially, the idea is to get stronger or leaner or more muscular. To facilitate these changes, the body must go through phasic adaptations regularly over time — in other words, you must train consistently. The basic underlying physiological response to regular training follows what’s known as the stimulus-fatigue-recovery-adaptation model (Figure 1).
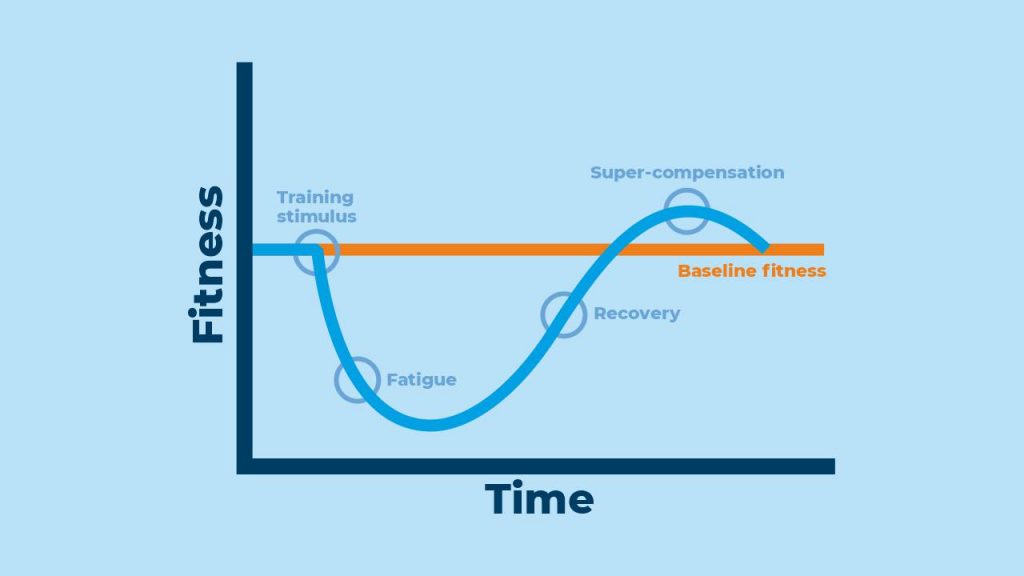
The phases of the stimulus-fatigue-recovery-adaptation model include:
- Lifting weights to supply a stimulus to the body
- The body then goes into the alarm phase, where fatigue levels increase
- The body then recovers, and tissue repair occurs
- The body then “super-compensates”, and there is a new training baseline that occurs, indicating your fitness has increased.
Importantly, during stages one and two, there is physical discomfort that occurs where the body tries to adjust to the training undertaken. This discomfort is caused by a number of biological processes to accommodate for physical change, and can often be misidentified as “bad pain”. But before we can understand the difference between good pain vs bad pain, we first need to understand what pain is and why it’s such an important mechanism.
What is pain?
Pain is an unpleasant sensory and emotional experience associated with tissue damage that is either real or perceived.
The pain response is complex, with the general concept relying on both your peripheral and central nervous systems to A) address what the pain is and B) manage the response to the pain — ie, how one should feel in response to it
For instance, pain can be instantly felt in the presence of immediate danger, whereby the pain receptors send a message to the spinal cord that prompts an involuntary reflex known as a reflex arc. Think about putting your hand on a hot stove, for example, whereby your reflex is to immediately pull away from the stove.
On the other hand, pain can also be felt chronically, whereby there is trauma via injury/ damage to muscle, or illness that causes long-lasting disruption to the pain processes. For example, suffering a stroke may cause what is called neuropathic pain, which means that the stroke has likely produced a disturbance in the somatosensory nervous system (the body’s pain system) that causes ongoing discomfort and requires considerable neurological and physical rehabilitation.
Pain can also be associated with exercise-induced muscle damage, commonly referred to as delayed-onset muscle soreness (DOMS). While the precise biological processes underlying DOMS needs further exploration, some hypotheses have been proposed.
One well-accepted hypothesis is that DOMS may be caused by muscle insult (ie, trauma resulting from resistance training), which triggers an inflammatory response due to microscopic tears in the connective tissue elements that sensitize the pain receptors called nociceptors surrounding the target muscle, thereby heightening the sensation of pain. DOMS may also be instigated by the presence of unstable molecules, known as reactive oxygen species, that lead to the degradation of proteins and ultimately apoptosis (cell death).
How do you know the difference between good pain (discomfort) and bad pain (injury)?
Is pain following exercise a good thing? Well, that really depends on the presentation of the pain. A key principle separating pain due to injury versus pain due to training-induced muscle microtrauma is the time of onset.
Pain because of muscle microtrauma may occur one to two days after training and can persist for several days
This particular type of pain can also present as a case of muscle discomfort and may lead to poor mobility and a feeling of general stiffness. Perceptions of such muscle discomfort can be wide-ranging, and severity may be based on the type of training undertaken.
For instance, DOMS is particularly common during routines that load up the muscle in its lengthened form or eccentrically. Furthermore, the level of pain/ discomfort experienced may also be dependent on one’s response to the training, which could vary depending on experience levels. Thus, beginner trainees are likely to be unaccustomed to resistance training, and so the initial pain response (due to more severe exercise-induced muscle damage) may be more pronounced. However, as physiological adaptation occurs over time following consistent resistance training, the pain response should diminish.
If pain occurs immediately — during or instantly following strength training — or is local in its presentation, ie, around a joint, or area of a muscle, then it is likely that there is underlying joint or muscle injury
There may also be other signs accompanying the immediate pain sensation, like signs of swelling at the site, loss of mobility, or loss in strength and power, which could also indicate muscle or joint injury.
On the other hand, if the pain is more global (for instance, “my thighs and arms are sore”), which may be reflective of DOMS, then it probably means your body is in the early stages of repair following resistance training, which is certainly a good thing. The body must change and grow somehow to the stimulus that has been supplied; that is how we adapt physiologically.
However, irrespective of training status, it must be noted that not everyone experiences the same level of pain. As such, DOMS severity may not always be a good indicator of exercise-induced muscle damage, nor how effective the repair process will be or how much physiological adaptation one will achieve.
How to reduce pain associated with DOMS
Both cold and heat applications post-exercise can be effective for reducing pain associated with DOMS, with no clear difference between the two therapies. Most of the evidence suggests that cold or heat application should occur within the one-hour window post-training for best results. However, this window could vary depending on the individual, as well as the length of time that pain (DOMS) is experienced.
In addition, massage and foam rolling may also be useful techniques for alleviating pain associated with DOMS post-exercise by increasing muscle blood flow and reducing muscle edema or swelling. For the time being, evidence is mixed (and contrasting) concerning the effectiveness of acupuncture for reducing pain from DOMS.
Also read: How Can You Recover From Workouts
Finally, if one is new to resistance training, employing exercises that target large muscles, and avoiding eccentric training, may also help to reduce the level of muscle damage — and pain — experienced post-training.
References
1. Leitzelar BN, Koltyn KF. Exercise and Neuropathic Pain: A General Overview of Preclinical and Clinical Research. Sports Med Open 2021; 7: 21.
2. Hainline B, Turner JA, Caneiro JP, et al. Pain in elite athletes-neurophysiological, biomechanical and psychosocial considerations: a narrative review. Br J Sports Med 2017; 51: 1259-64.
3. Hainline B, Derman W, Vernec A, et al. International Olympic Committee consensus statement on pain management in elite athletes. Br J Sports Med 2017; 51: 1245-58.
4. Schoenfeld BJ, Contreras B. Is postexercise muscle soreness a valid indicator of muscular adaptations? Strength & Conditioning Journal 2013; 35: 16-21.
5. Wang Y, Li S, Zhang Y, et al. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: A systematic review and meta-analysis of 32 randomized controlled trials. Phys Ther Sport 2021; 48: 177-87.
6. Chang WD, Chang NJ, Lin HY, et al. Effects of Acupuncture on Delayed-Onset Muscle Soreness: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med 2020; 2020: 5864057.
7. Huang C, Wang Z, Xu X, et al. Does Acupuncture Benefit Delayed-Onset Muscle Soreness After Strenuous Exercise? A Systematic Review and Meta-Analysis. Front Physiol 2020; 11: 666.
8. Dupuy O, Douzi W, Theurot D, et al. An Evidence-Based Approach for Choosing Post-exercise Recovery Techniques to Reduce Markers of Muscle Damage, Soreness, Fatigue, and Inflammation: A Systematic Review With Meta-Analysis. Front Physiol 2018; 9: 403.
9. Pearcey GE, Bradbury-Squires DJ, Kawamoto JE, et al. Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures. J Athl Train 2015; 50: 5-13.
Recommended